Chest auscultation is a straightforward but highly useful diagnostic technique that dates back to over 2,000 years ago.
What is Chest Auscultation?
Chest auscultation involves using a stethoscope to listen to a patient’s respiratory system and interpreting the lung sounds heard (Physiopedia 2015).
Auscultation is a fundamental component of physical examination that can assist in the diagnosis of respiratory issues. It is a non-invasive, safe procedure dating back to the era of Hippocrates (who used his ear rather than a stethoscope), making it one of the oldest diagnostic techniques (Physiopedia 2015; Sarkar et al. 2015; Proctor & Rickards 2020).
In addition to the respiratory system, auscultation can also be used to examine the heart, circulatory system and gastrointestinal system (Physiopedia 2015).
Despite being a fairly straightforward assessment, chest auscultation is a skill that requires considerable practice and understanding of the respiratory system so that you can differentiate normal respiratory sounds from abnormal and adventitious sounds (e.g. sibilant wheezes and crackles), to accurately diagnose patients (Sarkar et al. 2015).
The more lung sounds you listen to, the easier it will be to identify an abnormality and report it to a member of the medical team.
It is important to remember that auscultation is just one component of respiratory assessment; ensure you also monitor the rise and fall of the patient’s chest and identify any potential difficulties they may be experiencing (shallow breathing, pain, use of accessory muscles, reduced ability to follow instructions, sputum production, asymmetry of the chest etc.).
Chest auscultation should be contextualised to a patient’s medical history and form one component of a holistic assessment (Proctor & Rickards 2020).
What are Lung Sounds?
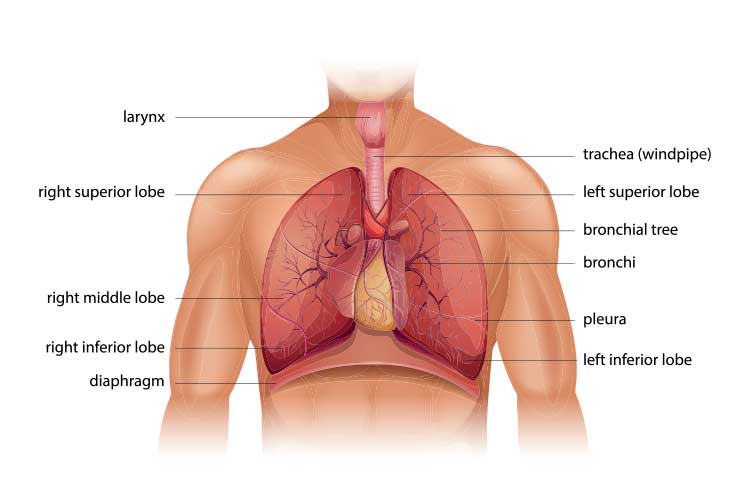
Lung sounds are caused by vibrations of the vocal cords during inspiration and expiration, which are transmitted to the trachea and bronchi. These sounds can be used to monitor airflow through the trachea and bronchial tree (Proctor & Rickards 2020).
Problematic lung sounds may be abnormal (meaning they are absent, sound different to normal sounds or are heard in a different location to what is normal) or adventitious (additional sounds that are heard over the top of regular sounds) (Prakash et al. 2015).
Lung sounds are caused by vibrations of the vocal cords during inspiration and expiration, which are transmitted to the trachea and bronchi.
Ideally, chest auscultation should be performed on all patients as part of a head-to-toe assessment. This will ensure you have adequate insight into a patient’s condition at the commencement of your shift and will be able to escalate care if any deterioration is identified.
Other situations where chest auscultation may be used include:
Patient deterioration (or early detection of deterioration)
Suspected fluid overload
Respiratory conditions
Cardiac conditions
Heart failure
On admission to hospital
Admittance of an intensive care unit patient back to the ward
Baseline assessment at shift commencement
Before surgery (perioperatively)
After surgery (postoperatively)
Intraoperatively (by the anaesthetic nurse or doctor)
After extubation and intubation in critical care settings.
(Tsotsolis et al. 2015; Prakash, Mullick & Pawar 2015)
How to Perform Chest Auscultation
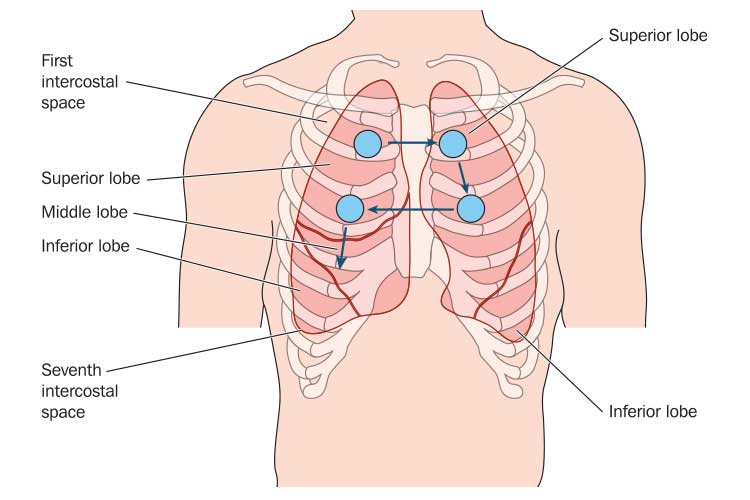
Place the diaphragm of the stethoscope flat on the patient’s chest at several points, following the stepladder pattern.
Prepare a quiet environment so that you will be able to clearly hear the patient’s lung sounds.
Ensure the patient is haemodynamically stable before mobilising them.
Ensure the patient’s pain (if any) has been adequately treated. Consider analgesia if needed.
Ensure all lines and drains are positioned safely when mobilising the patient.
Sit the patient in a chair or upright on the side of the bed if possible.
Consider PPE precautions if required (always follow your organisation’s policies and procedures).
Ensure you have a clean, designated stethoscope for the patient.
The assessment requires the patient’s chest and back to be exposed - ensure the patient’s privacy and dignity is maintained.
Using gentle pressure, place the diaphragm (chest piece) of the stethoscope flat on the patient’s chest.
Listen to lung sounds on the anterior chest using the ‘stepladder’ pattern. At each point, you should ensure the diaphragm stays in contact with the chest for one full inspiration and expiration cycle.
Repeat this process for the posterior chest (avoiding the scapula).
Listen to the patient’s right lateral chest (they will need to move their right arm out of the way). Listen to the upper lobe, then the middle lobe, then the lower lobe.
Repeat this process for the left lateral chest (there is an upper and lower lobe only).
If the patient becomes dizzy, call for help. Put the patient back into bed immediately or lower them onto the floor safely.
If the patient’s intravenous or central line dislodges due to mobilisation, call for assistance.
If the patient becomes haemodynamically unstable, place them in a safe position on the bed or floor, adhering to safe manual handling practices.
If the patient experiences sudden or severe difficulty breathing or stops breathing, this is an emergency. Perform a respiratory assessment and commence basic life support if required.
Conclusion
Chest auscultation is an important component of respiratory assessment. By having a baseline of the patient’s condition, you should be able to recognise any early signs of deterioration.
Ensure you familiarise yourself with lung sounds, as the more you practice, the better you will become at identifying abnormalities.
 New
New