Exposure Prone Procedure (EPP) Risks in Healthcare
CPDTime.
11m
Updated 09 Feb 2025
Healthcare workers are responsible for protecting their patients’ health and safety. This includes preventing the transmission of bloodborne viruses, particularly when performing exposure prone procedures (EPPs).
This commitment must be made upon initial registration. At each renewal, the practitioner must state that they did comply with the CDNA guidelines in the previous registration period and will commit to complying again in the next registration period (NMBA 2021).
What are Exposure Prone Procedures?
Exposure prone procedures (EPPs) are medical processes where there is potential for the healthcare worker to become injured and bleed into a patient’s open tissues (CDNA 2019).
EPPs involve the HCW’s hands (gloved or ungloved) making contact with sharp instruments, needle tips or sharp tissues such as teeth inside a patient’s open body cavity, wound or confined anatomical space where the HCW’s hands or fingertips are not completely visible throughout the procedure (CDNA 2017).
Procedures that are not considered EPPs are those where:
The HCW’s hands are visible and outside of the patient’s body at all times, or
There is no potential for the HCW’s hands to be injured by sharp instruments or tissue.
(CDNA 2017)
Note that some non-EPP procedures may escalate and will require a professional who is appropriately qualified to perform EPPs (CDNA 2017).
The major risk associated with EPPs is that HCWs may transmit certain bloodborne viruses to their patients (or vice versa) if their blood comes into contact with the patient’s open tissues (CDNA 2019).
1% to 62% (depending on the patient’s hepatitis B e-antigen status)
Hepatitis C virus
Blood
Body fluid contaminated with blood
0.04% to 4.35%
0% to 7%
Human immunodeficiency virus (HIV)
0.0000024% to 0.000024%
0.3%
(Adapted from CDNA 2019)
There have only been four cases worldwide of HIV transmission to patients during EPPs. In all of these cases, the HCW was not taking antiretroviral therapy (CDNA 2019).
Recommendations for Healthcare Workers
In general, all HCWs should be aware of their BBV status and take reasonable precautions to avoid transmission. Those who are at risk of contracting a BBV outside of work should seek regular testing (CDNA 2017).
Furthermore, all HCWs (including students) are expected to be vaccinated against hepatitis B before commencing their employment (CDNA 2017).
Those who perform EPPs should be tested for bloodborne viruses at least once every three years and should seek follow-up care and testing in a timely manner if they have potentially been exposed to a BBV occupationally or outside of work (CDNA 2018).
BBVs may be asymptomatic or mild, meaning that a HCW who has not been tested may not be aware that they have contracted a BBV (CDNA 2018).
Risk Factors for Blood or Body Fluid Exposure
Being injected with over 1 mL of blood or body fluid
Parenteral exposure to laboratory specimens containing a high concentration of a BBV
Suffering a skin-penetrating injury, including:
Injury from a needle that is contaminated with blood or body fluid
Injury that results in bleeding and is caused by an instrument that is visibly contaminated with blood or body fluid
Injury that causes the mucous membrane or conjunctival contact to come into contact with blood
Injury from a human bite or scratch where there is exposure to blood or body fluid infectious for a BBV
Direct contact between non-intact skin and blood or body fluid
Direct vaccination with HIV tissue or material, or material likely to contain HIV, HBV or HCV (in laboratory settings).
(Queensland Health 2024)
Management of Exposures to Blood and Body Fluid
If you are exposed to blood or body fluid, immediate steps should be taken:
Note: Always adhere to your organisation’s policies and procedures.
Wash any skin areas (including wounds and non-intact skin) that have come into contact with blood or body fluid using soap and water.
Avoid squeezing or rubbing the affected area.
If the eyes or mucous membranes have been exposed:
Irrigate using water or normal saline
If the eyes are contaminated, rinse them while open for at least 30 seconds (remove any contact lenses first).
If blood or bodily fluids have entered the mouth, spit them out and rinse the mouth out with water multiple times, spitting the water out each time.
Remove any contaminated clothing and shower if required.
(Queensland Health 2024; SA Health 2023)
Documentation is crucial after an incident of exposure has occurred. It should include:
Information about the exposure:
Date and time of the exposure
Type of exposure, including site, blood or body fluid involved, and first aid performed
Type of injury sustained from the incident
Information about the object that caused the injury (e.g. the gauge of the needle)
Type of body fluids involved
The volume of blood or body fluid the person was exposed to
Information about the source person:
BBV status
Demographic factors that may increase the risk of BBV infection
Information about the exposed person:
Status of the exposed person with respect to BBVs, including vaccination status
Pregnancy risk and lactation
Medical history.
(Queensland Health 2024)
What Happens if a Healthcare Worker Tests Positive for a Bloodborne Virus?
A HCW who tests positive for a BBV must stop performing EPPs immediately (CDNA 2017).
They will be allowed to resume performing EPPs if they:
Seek ongoing and appropriate medical care for the BBV
Undergo testing for viral load levels
Maintain viral load levels that comply with the criteria stated in CDNA Guidelines
Undergo any required treatment as stated in the CDNA Guidelines, and
Comply with other relevant criteria as stated in the CDNA Guidelines.
(CDNA 2017)
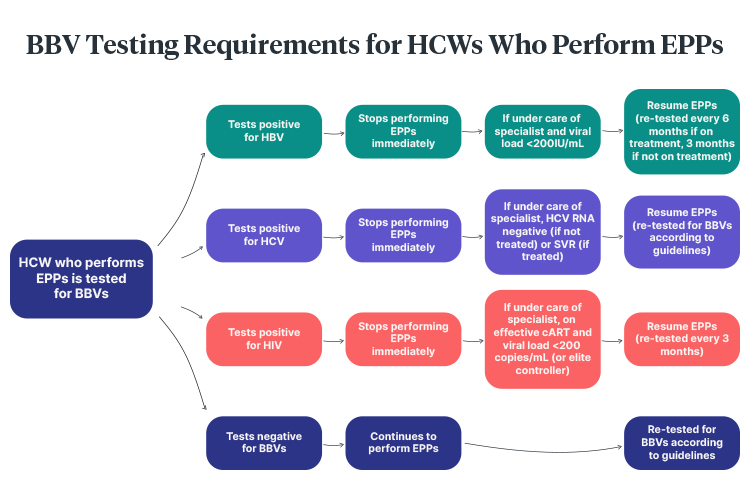
The pathway for resuming EPPs after a BBV diagnosis is as follows:
Note: Always adhere to your organisation’s policies and procedures.
(Adapted from CDNA 2019)
Note: False positives for BBV are possible but very rare, as screening involves a two-step testing process (CDNA 2017).
Patient Exposure to Blood or Body Fluid From a Healthcare Worker With a BBV
Note: Always adhere to your organisation’s policies and procedures.
If this occurs, a comprehensive risk assessment should be performed in consultation with the HCW’s treating practitioner. This risk assessment should comprise:
The significance of the exposure
The exposed patient’s status
The HCW’s BBV status, including:
Current viral load
BBV history
Adherence to treatment
Frequency and severity of fluctuations in viral load
Any factors that might increase viral load.
(CDNA 2019)
If there is any concern that the HCW’s viral load is above the allowed level, the HCW should be tested immediately. Post-exposure prophylaxis and any other follow-up should be offered to the patient based on local policies (CDNA 2019).
Test Your Knowledge
Question 1 of 3
Which one of the following is an exposure prone procedure?
 New
New