Hypokalaemia commonly develops in hospital settings. While it is generally mild, it can cause serious complications if not addressed.
What is Hypokalaemia?
Hypokalaemia is a common electrolyte imbalance that presents in about 20% of hospitalised patients, characterised by lower than normal levels of potassium in the serum blood (Kardalas et al. 2018).
Hypokalaemia is reversible and generally asymptomatic unless the patient’s potassium levels are extremely low (Rogers 20216).
What is the Role of Potassium in the Body?
Potassium contributes to the functioning of nerve and muscle cells, particularly the muscle cells in the heart. Potassium is regulated by the kidneys to maintain homeostasis within a tight range, with excess expelled through urine, sweat and gastrointestinal losses (Rogers 2016; Castro & Sharma 2020).
A loss of homeostasis will result in either hypokalaemia or hyperkalaemia (excess potassium levels), both of which can cause adverse effects (Lewis 2020).
Potassium plays a particularly important role in cardiac action potential and electrophysiology. When there is an imbalance, the myocardium is unable to pump effectively due to a disruption in the electrical conduction. This results in arrhythmias that may be induced by low potassium levels. This can be life-threatening if not detected early, requiring critical care services (Weiss, Qu & Shivkumar 2017).
Potassium, which can be found in several foods, contributes to the functioning of nerve and muscle cells, particularly the muscle cells in the heart.
Levels of Hypokalaemia
Hypokalaemia is defined as any potassium level below 3.5 mmol/L (millimoles per litre) (Lewis 2020).
A normal range of potassium is 3.5 mmol/L to 5.2 mmol/L.
Mild hypokalaemia is defined by potassium levels of 3.0 to 3.5 mmol/L.
Moderate hypokalaemia is defined by potassium levels of 2.5 to 3.0 mmol/L.
Critical hypokalaemia is defined by potassium levels of less than 2.5 mmol/L.
(NSW DoH 2016)
Note: Some ranges may vary depending on hospital protocols.
It is also important to identify the cause of the patient’s hypokalaemia. This may be straightforward if the patient is displaying symptoms that suggest excessive potassium loss (e.g. vomiting), or taking medicines that cause potassium loss (Lewis 2020).
Treating Hypokalaemia
Notify the medical team.
Reassure the patient and explain what is happening.
Ensure the patient is in bed.
Take the patient’s observations (vital signs) and conduct a head-to-toe assessment.
Review the patient’s medication chart (e.g. check for any diuretics that may be documented).
Increase the frequency of observations.
Review the patient’s blood tests.
Consider continuous cardiac monitoring.
Identify and remove the underlying cause of the hypokalaemia.
Correct the patient’s electrolyte imbalances as per your organisation’s protocol and medical advice, taking into account the severity of the hypokalaemia.
Consider intensive care admission if the patient is haemodynamically unstable.
Undertake regular serum potassium checks.
(ECI 2017; Tidy 2017)
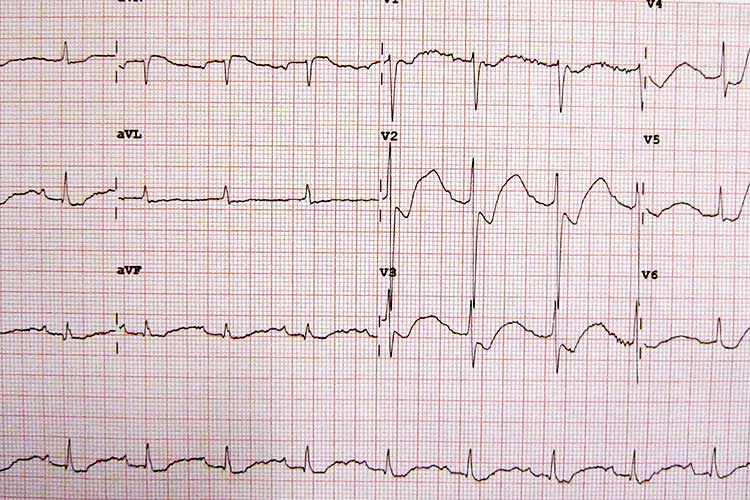
An ECG is recommended in moderate or severe cases (or mild cases in a high-risk patient) to check cardiac function and ensure the heart has not been compromised. Potassium is vital for cardiac action potential and electrophysiology (Tidy 2017).
Preventing Hypokalaemia
As hypokalaemia mostly develops in hospital settings, you should conduct monitoring such as accurate fluid balance charts to ensure that potassium levels are optimised and any imbalances can be restored (Rogers 2016).
Complications of Hypokalaemia
Cardiac arrhythmias and acute respiratory failure caused by paralysis are the most serious complications of hypokalaemia and can be life-threatening if not addressed early (Lederer 2018).
If intravenous administration is required, administer it slowly and be mindful that it may be painful to the patient. Rapid correction of hypokalaemia may result in cardiac arrest. Always follow your organisation’s protocol (NSW DoH 2014; QLD DoH 2016).
Hyperkalaemia (the opposite condition to hypokalaemia wherein there is excessive potassium in the body) can also be life-threatening in severe cases (National Kidney Foundation 2016). Therefore, take care when administering potassium to a patient with hypokalaemia in order to reduce the risk of ‘rebound’ hyperkalemia (Castro & Sharma 2020).
If intravenous administration is required, always follow your organisation’s protocol.
Conclusion
Hypokalaemia is reversible and generally mild but can be life-threatening if potassium drops to critical levels. It is important to understand the role potassium plays in the body and ensure it is always optimised. If you are required to administer potassium to a patient, always do so safely and refer to your organisation’s protocol.
Note: This article is intended as a refresher and should not replace best-practice care. Always refer to your facility's policy on hypokalaemia.
Zhu, Q et al. 2018, ‘Prevalence and Risk Factors for Hypokalemia in Patients Scheduled for Laparoscopic Colorectal Resection and its Association With Post-operative Recovery’, BMC Gastroenterology, vol. 18 no. 1, viewed 21 May 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6194555/
Test Your Knowledge
Question 1 of 3
How would you diagnose a patient with a potassium level of 3.2 mmol/L?
Topics
For Teams
Assign to your staff
Assign mandatory training and keep all your records in-one-place.
 New
New