Otitis Media and Myringotomy in Aboriginal and Torres Strait Islander Children
CPDTime.
6m
Updated 10 May 2021
What is Otitis Media?
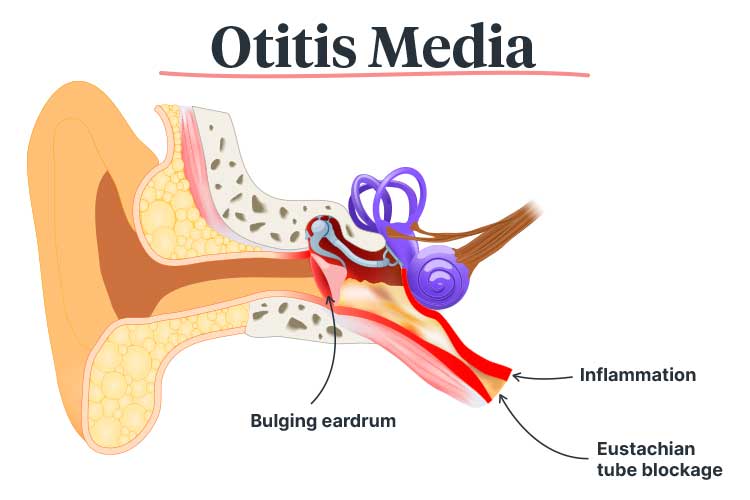
Otitis media is an umbrella term encompassing all types of inflammation and infection of the middle ear, which is the air-filled, membrane-lined cavity located behind the eardrum (CRE_ICHEAR 2016; Children’s Health Queensland 2019; Healthline 2018).
People of all ages can be affected by otitis media, but it is most common among young children, especially those between 6 and 18 months of age. It is estimated that about 75% of children will have experienced at least one episode of otitis media by the time they start school (Healthdirect 2020; RCHM 2020).
In most cases, otitis media arises from a viral or bacterial infection that initially presents as a cold. The infection may then spread to the middle ear through the eustachian tube, causing swelling and a build-up of fluid. As this places pressure on the eardrum, there is a risk that the eardrum will perforate (burst) (Healthdirect 2020).
Risk Factors for Otitis Media in Children
Children who are at increased risk of otitis media include:
Aboriginal and Torres Strait Islander children
Children of low socio-economic status
Immunocompromised children
Children living with Down’s syndrome
Children who attend daycare
Children who use a dummy
Children who are exposed to cigarette smoke.
(PCH 2021; Children’s Health Queensland 2019)
Symptoms of Otitis Media
Generally, initial symptoms will be those of a cold, including a sore throat, runny nose and fever. When the infection spreads to the ear, symptoms may include:
Ear pain
Headache
Fever
Impaired hearing
Crying
Pulling or rubbing at the ears
Irritability
Loss of appetite
Fluid or blood drainage from the ear (if the eardrum has perforated).
(Healthdirect 2020; Children’s Health Queensland 2019)
Types of Otitis Media
The main presentations of otitis media are:
Acute Otitis Media
Acute otitis media (AOM) is a painful infection of the middle ear, often with a sudden onset. It may be accompanied by fever, fluid in the middle ear, irritability and a red eardrum bulging with pus (ACSQHC 2021a; SCHN 2020).
AOM is one of the most common causes of severe pain in children, with almost every person experiencing at least one episode during their childhood (ACSQHC 2021a; PCA 2021).
Otitis Media With Effusion
Otitis media with effusion (OME), which is also known as glue ear, is characterised by a build-up of fluid in the middle ear (ACSQHC 2021a; SCHN 2020).
OME is not an acute infection. It often occurs when fluid accumulates in the middle ear and eustachian tube following a cold or episode of AOM. Generally, the only symptom of OME is hearing impairment due to the fluid obstruction (SCHN 2020). The condition is not painful but may cause annoyance. As the signs of OME are subtle, it is easy to overlook (ACSQHC 2021a).
Most episodes of OME will resolve on their own within three months. However, 25% of children will experience ongoing OME, and consequently, persistent hearing interference. This may lead to difficulties with language, education and behaviour (ACSQHC 2021a).
A child with OME may display the following behaviours:
Rubbing or pulling their ears
Lack of attention or constantly replying ‘what?’ to others
Speech delay
Turning the television volume up
Not ‘listening’
Difficulties with balance.
(SCHN 2020)
Chronic Suppurative Otitis Media
Chronic suppurative otitis media (CSOM), also known as runny ear, describes chronic (for two and six weeks) drainage of ear discharge through a perforation (hole) in the eardrum (i.e. tympanic membrane) (ACSQHC 2021a; Rosario & Mendez 2021).
CSOM may arise as a complication of AOM if the pressure caused by swelling and fluid perforates the eardrum (Healthdirect 2020). Other potential causes include eustachian tube obstruction, ear injuries and blast injuries (Miyamoto 2020).
Discharge will drain profusely and may be white, yellow or green. In most cases, it is not painful or accompanied by inflammation, but may have a foul smell. CSOM that has persisted for a long time is likely to contain multi-resistant pathogens. It is a difficult condition to treat (PCH 2021; Miyamoto 2020).
CSOM is the most disabling type of otitis media and is difficult to treat. Drainage may continue for years and may even lead to permanent hearing loss (ACSQHC 2021a; PCH 2021).
Treatment of Otitis Media
Treatment of otitis media generally involves symptom management using analgesics. Bacterial infections may be treated with antibiotics (Children’s Health Queensland 2019).
In most cases, otitis media will resolve on its own (ACSQHC 2021a).
Otitis Media in Aboriginal and Torres Strait Islander Children
Otitis media is a significant issue affecting Aboriginal and Torres Strait Islander children, who have the highest rate of middle ear disease in the world. They are also more likely to experience earlier, more severe and longer-lasting middle ear disease than non-Aboriginal and Torres Strait Islander children (ACSQHC 2021a).
In fact, a report published in the Medical Journal of Australia in 2021 found that in remote Northern Territory communities, only 1 in 10 Aboriginal children under the age of three have healthy ears, while 5 in 10 have OME and 4 in 10 have CSOM (Leach et al. 2021).
The rate, frequency and severity of otitis media in Aboriginal and Torres Strait Islander children is comparable to that of children living in developing countries (DeLacy, Dune & Macdonald 2020).
Aboriginal and Torres Strait Islander children who experience hearing loss within their first 1,000 days of life are at risk of delayed speech and language development, which may lead to issues that carry into adulthood (ACSQHC 2021a; NSW Health 2018). These include:
Education difficulties
Impaired language development and speech issues
Vulnerability upon starting school
Inattention
Non-attendance at school
Early school leaving
Social isolation
Reduced education and employment opportunities.
(ACSQHC 2021a; Leach et al. 2021)
Risk Factors for Otitis Media in Aboriginal and Torres Strait Islander Children
The prevalence of otitis media in Aboriginal and Torres Strait Islander communities is associated with social determinants of health and environmental factors, including:
Overcrowded housing, which has been identified as the most significant risk factor for ‘upper respiratory tract carriage’
Poor housing conditions
Exposure to cigarette smoke
Socioeconomic disadvantage
Poverty and low income
Difficulty accessing health services
Poor hygiene
Lack of education
Unemployment and lack of employment opportunities
Malnutrition
Lack of community involvement in service provision and planning
Cultural and language differences
Premature birth
Being bottle-fed, especially ‘prop feeding’ wherein the bottle is propped up so that the infant can feed without supervision, or if the infant falls asleep with a bottle in their mouth.
(DeLacy, Dune & Macdonald 2020; NSW Health 2018; Whalan 2019)
What is Myringotomy?
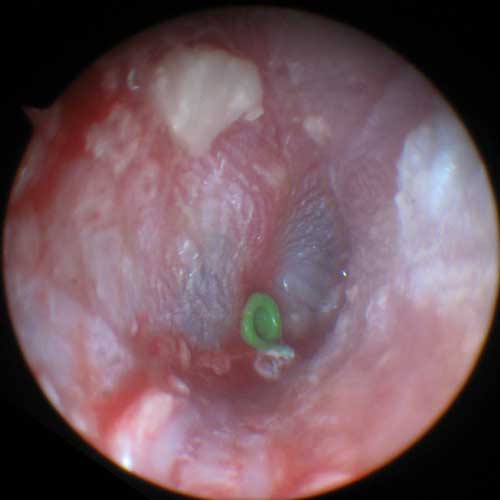
Grommets are often inserted during myringotomy to ensure the incision stays open.
Myringotomy is a surgical procedure used to treat otitis media wherein a small incision is made in the eardrum in order to drain discharge from the middle ear. Grommets (tympanostomy tubes) are often inserted to ensure the incision stays open, facilitating ventilation and drainage (ACSQHC 2021a).
What are the Benefits of Myringotomy?
While myringotomy is generally not a first-line treatment for AOM or OME, it may be beneficial in some situations. Clinical practice guidelines recommend myringotomy for children who have been experiencing OME in both ears for longer than three months and have documented hearing loss. The more severe the hearing loss, the more likely myringotomy is to be beneficial to the child (ACSQHC 2021a).
Furthermore, myringotomy is potentially effective in reducing recurrent ASOM episodes, however, more evidence is needed. Clinical practice guidelines in the United States recommend the procedure for children who have experienced:
Three episodes of AOM in six months, or
Four episodes of AOM in one year.
(ACSQHC 2021a)
Generally, grommets should only be inserted if OME is also present. Whether grommets are more effective than antibiotics in reducing recurrent AOM is still uncertain (ACSQHC 2021).
Potential Complications of Myringotomy
Discharge through the grommets, which affects about 25% of children
Eardrum perforation.
(ACSQHC 2021a)
Myringotomy in Australia
Myringotomy with grommet insertion is one of the most common paediatric surgical procedures in Australia, especially for those aged between 0 and 4 years of age (ACSQHC 2021a).
Despite this, according to the Fourth Australian Atlas of Healthcare Variation, Aboriginal and Torres Strait Islander children receive less myringotomy than what is expected based on the prevalence of otitis media in Aboriginal and Torres Strait Islander communities (ACSQHC 2021b).
This suggests that:
Some Aboriginal and Torres Strait Islander children who would benefit from myringotomy do not receive it
Some non-Aboriginal or Torres Strait Islander children are undergoing myringotomy despite not needing it.
(ACSQHC 2021b)
How Can Otitis Media Care in Aboriginal and Torres Strait Islander Children be Improved?
According to the Atlas, a ‘comprehensive community approach’ is required in order to improve the prevention, diagnosis and treatment of otitis media in Aboriginal and Torres Strait Islander children (ACSQHC 2021b).
One important consideration is Aboriginal and Torres Strait Islander communities’ holistic approach towards health, which includes ‘body, mind, spirit, land, environment, custom, socioeconomic status, family and community’ and differs from the ‘mainstream’ approach (DeLacy, Dune & Macdonald 2020).
Strategies that may help to reduce the prevalence of otitis media in Aboriginal and Torres Strait Islander communities include:
Encouraging breastfeeding rather than bottle-feeding
Ensuring children get adequate nutrition
Ensuring children have safe and healthy housing conditions
Ensuring children are up-to-date with their immunisation schedule
Medical services providing patient and community education, screening and smoking cessation advice in a culturally appropriate way
Newborn hearing screening.
(NSW Health 2018; Liotta 2018)
Furthermore, strategies should be put into place to ensure that Aboriginal and Torres Strait Islander children who require myringotomy are able to receive it. These include:
Improving the monitoring of ear health
Improving training in the diagnosis of middle ear disease
Updating relevant guidelines
Improving Aboriginal and Torres Strait Islander peoples’ ability to access hearing support services and audiologists
Improving Aboriginal and Torres Strait Islander peoples’ ability to access ear, nose and throat specialists
Leach, A J et al. 2021, ‘Otitis Media Guidelines for Australian Aboriginal and Torres Strait Islander Children: Summary of Recommendations’, Medical Journal of Australia, vol. 214, no. 5, viewed 5 May 2021, https://onlinelibrary.wiley.com/doi/10.5694/mja2.50953
 New
New