This article will discuss how to assess acute pain in critically ill patients.
Pain should be predicted in all patients, and every action should be questioned for its possibility of causing pain or discomfort. Anticipating pain allows alternative strategies to be considered or pre-emptive analgesics given (Mallet et al. 2013).
What is Pain?
Pain is defined as ‘An unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage’ (IASP 2020).
Causes of Pain in Critically Ill Patients
Between 40 and 77% of critically ill patients admitted to intensive care units are estimated to experience moderate to severe pain (Bhattacharyya et al. 2023).
Pain often occurs at rest and during standard care procedures, and can lead to adverse outcomes such as stress responses, cognitive impairment, impaired sleep and agitation (Seo et al. 2022).
Potential causes of pain in critically ill patients can include:
Surgery
Trauma
Invasive procedures
Intubation and extubation
Nasogastric tubes
Mechanical ventilation
Nursing care such as repositioning, bathing and changing sheets
Endotracheal suctioning
Insertion of arterial lines, peripheral IVs and central venous catheters
Drains/drain removal
Peripheral blood draws
Respiratory exercise
Eye and mouth care
Mobilisation.
(Pandharipande & Hayhurst 2024; Seo et al. 2022; Devlin et al. 2018)
Pain is often underreported in critically ill patients (Pandharipande & Hayhurst 2024). Therefore, patients should be assessed for pain regularly, and the frequency of assessment should be patient-specific and adjusted according to their risk.
Potential Barriers to Adequate Pain Management in Critically Ill Patients
A qualitative study by Bhattacharyya et al. (2023) identified several potential barriers to adequate pain management in ICU settings, including:
Lack of knowledge of and/or trust in pain assessment tools
High clinical workloads
Pain not being viewed as a priority in critically ill patients
Biases and assumptions of pain levels based on demographic factors (e.g. age, ethnicity)
Lack of confidence in pain management abilities
Difficulty communicating with patients who are sedated and/or experiencing delirium
Concerns related to high-dose use of opioids.
The Effects of Untreated or Unmanaged Pain
Untreated pain can pose serious consequences for the already compromised critically ill patient, potentially leading to both short and long-term physical and psychological consequences such as:
Stress responses, including tachycardia, hypercoagulation, respiratory compromise, immunosuppression, catabolism and increased myocardial oxygen consumption
Increased length of stay in the ICU
Increased duration of mechanical ventilation
Wound infection
Impaired sleep
Exhaustion
Disorientation
Agitation
Chronic pain
Post-traumatic stress disorder (PTSD).
(Bhattacharyya et al. 2023; Seo et al. 2022)
Pain Assessment in the Critically Ill Patient
Careful consideration needs to be given to the assessment method chosen for critically ill patients because they are often unable to participate in the pain assessment process.
Below are some methods of assessing pain in critically ill patients:
Self-Report Tools
Self-report is considered the most reliable method of pain assessment (Health.vic 2024)
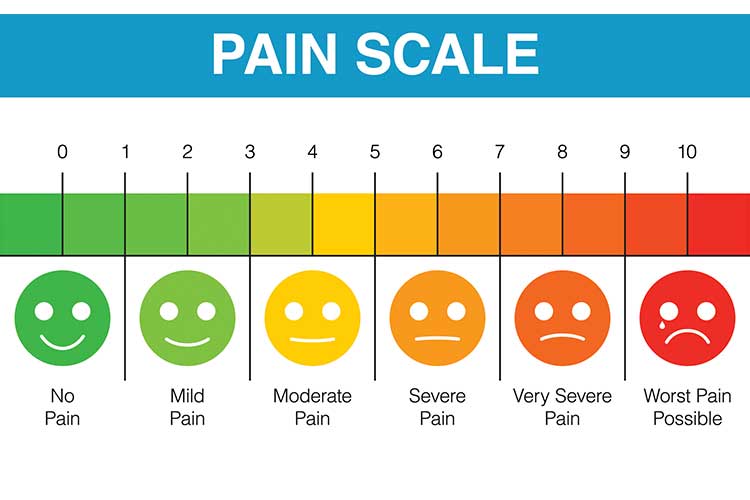
This method is offered to patients who are able to communicate, even if not verbally. A numerical rating scale (NRS) with a standard scale of 0-10 (where 0 = pain-free and 10 = worst pain you can imagine) can still be used if the patient is able to point to the scale or nod at simple commands (Nordness et al. 2021).
Other examples of self-report assessment tools include the verbal description scale (VDS) and the visual analogical scale (VAS)
Observational Tools
You may be unable to obtain a self-report from some critically ill patients due to factors such as sedation or delirium. In these cases, an observation of the patient’s pain behaviours can be used to measure pain instead (Chanques & Gélinas 2022).
The most reliable pain assessment tools for critically ill patients who cannot self-report are the behavioural pain scale (BPS) and the critical care observation pain tool (CPOT) (Seo et al. 2022).
The Behavioural Pain Scale (BPS)
Facial expression
Relaxed
+1
Partially tightened (e.g. brow lowering)
+2
Fully tightened (e.g. eyelid closing)
+3
Grimacing
+4
Upper limb movement
No movement
+1
Partially bent
+2
Fully bent with finger flexion
+3
Permanently retracted
+4
Compliance with mechanical ventilation
Tolerating movement
+1
Coughing, but tolerating ventilator for most of the time
+2
Fighting ventilator
+3
Unable to control ventilation
+4
(Adapted from Seo et al. 2022)
The scores from each of the three sections are added together:
No pain
≤ 3
Mild pain
4-5
Unacceptable amount of pain
6-11
Maximum pain
≥ 12
(Adapted from MDCalc n.d.)
Typically, a score of ≥6 indicates sedation and/or analgesia.
The Critical Care Observation Pain Tool (CPOT)
Facial expression
No muscular tension observed
Relaxed, neutral
+0
Presence of frowning, brow lowering, orbit tightening and levator contraction
Tense
+1
All of the above facial movements plus eyelid tightly closed
Grimacing
+2
Body movement
Does not move at all (does not necessarily mean absence of pain)
Absence of movements
+0
Slow, cautious movements, touching or rubbing the pain site, seeking attention through movements
Protection
+1
Pulling tube, attempting to sit up, moving limbs/thrashing, not following commands, striking at staff, trying to climb out of bed
Restlessness
+2
Muscle tension: evaluating by passive flexion and extension of upper extremities
No resistance to passive movements
Relaxed
+0
Resistance to passive movements
Tense, rigid
+1
Strong resistance to passive movement, inability to complete them
Very tense or rigid
+2
Compliance with the ventilator (intubated patients) OR
The total score of the CPOT will be between 0 and 8, where 0 ≤ 2 indicates no pain and > 2 indicates pain and the need for analgesia (Nazari et al. 2022).
Conclusion
Effective pain assessment is an important element of the nurses’ role. The effects of inadequate pain management are significant and can lead to delayed healing and prolonged recovery. The nurse, therefore, must be competent in pain assessment methods in order to identify pain in critically ill patients so that appropriate analgesia can be administered.
Test Your Knowledge
Question 1 of 3
Which one of the following tools can be used to assess pain in critically ill patients who cannot self-report?
Nazari, R et al. 2022, ‘Diagnostic Values of the Critical Care Pain Observation Tool and the Behavioral Pain Scale for Pain Assessment among Unconscious Patients: A Comparative Study’, Indian J Crit Care Med., vol. 26, no. 4, viewed 1 August 2024, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9067504/
Nordness, MF, Hayhurst, CJ & Pandharipande, P 2021, ‘Current Perspectives on the Assessment and Management of Pain in the Intensive Care Unit’, J Pain Res., vol. 14, viewed 1 August 2024, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8214553/
Seo Y, Lee H, Ha EJ & Ha TS 2022, ‘2021 KSCCM Clinical Practice Guidelines For Pain, Agitation, Delirium, Immobility, and Sleep Disturbance in the Intensive Care Unit’, Acute Crit Care., vol. 37, no. 1, viewed 31 July 2024, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8918705/
For Teams
Assign to your staff
Assign mandatory training and keep all your records in-one-place.
 New
New